


After the full-text screening and evaluation for eligibility, 120 publications were included in the scoping review. Additionally, citation tracing was performed by reviewing reference lists of the retrieved full-text articles and looking up the papers that cite the retrieved articles. This resulted in 9 additional articles included in the scoping review. For the PRISMA flowchart illustrating the process of eligibility screening, see Additional file 2.
The review included 129 articles and book chapters (see Additional file 3 for the full list of the included articles and book chapters). The articles represent a wide range of fields of research—clinical psychology, general medicine, neuroscience, genetics, clinical genetics, psychiatry and mental health, philosophy, ethics, etc. The majority of the articles (83) are theoretical studies, 35 papers report results of empirical research and 11 are review papers. The distinction between review papers and theoretical papers, however, is blurred. The earliest paper was published in 1989, the latest—in 2023. To determine the most influential papers in the set several measures were used. The list of most global cited documents (Table 1) shows the papers that have received the most citations in total.
This, however, does not mean that these are the most relevant studies on the topic of the review. For example the by far the most cited paper is by Graham et al. (23). It is an overview of the current applications of AI in healthcare and the recent research of AI specific to mental health. Therefore, the high number of citations might (at least partly) be explained by the wide area of topics it addresses and by the recent surging interest in psychiatric AI applications. The same applies to the article by Chekroud et al. (24). It is also worth to notice that all papers (except Meiser et al.) in the Table 1 are published in journals on psychiatry (Current Psychiatry Report, World Psychiatry, Schizophrenia Research, JAMA Psychiatry, Journal of Affective Disorders) and genetic research (European Journal of Human Genetics) and not, for example, in the field of bioethics or sociology of medicine. The citation count differs across disciplines and papers in life sciences are in general more cited than papers in social sciences or humanities (25). This at least partly explains the absence of bioethics papers in Table 1. Alternatively, we investigated the list of most locally cited documents, i.e., the papers that are most often cited by other papers that we selected for the review (Table 2).
Table 2 lists ten most cited papers within the collection of articles that we included in the review. As we see, some papers have disappeared (e. g. Graham S, 2019; Fusar-Poli P, 2021; Chekroud AM, 2021), some improved their position (e.g. Corcoran C, 2005; Meiser B, 2005) and some new papers made the list (e.g. Laegsgaard MM, 2008; Hoge SK, 2012). Interestingly a couple of papers that are published in bioethics journals appear in the list as well (Lawrence RE, 2016; Mittal VA, 2015). This list of most locally cited papers has a better chance to represent the list of most influential papers on the topic of the review as it includes the papers that are more focused on the topic of our interest. However, provided the various limitations (e.g. the differences in citation practices between disciplines, the bibliometric analysis is based only on that data from SCOPUS) this claim should be taken with some reservations.
To get additional insight into the relations between the articles and themes that are covered in them, we utilised VOSViewer to produce a map of bibliographic coupling relations (Fig. 1). Bibliographic coupling tracks relations between the documents. Two papers are bibliographically coupled if there is a third paper that is cited by both papers—“bibliographic coupling is about the overlap in the reference lists of publications. The larger the number of references two publications have in common, the stronger the bibliographic coupling relation between the publications” (20). The idea behind bibliographic coupling is that two publications sharing common references are also similar in their content (26). The bibliographic network in Fig. 1 consists of nodes (dots) and edges (connections between dots). The diameter of the nodes and the thickness of the edges corresponds to the number of the links that the item has with other items. Further, the location of a node is determined by relations of a paper to other documents. There are 107 nodes in the map in Fig. 1 (to reduce the noise, the minimum number of citations of a document was set to 5) and setting the resolution parameter to 1, VOSviewer algorithm assigned the papers into a network of six clusters that are represented by different colours.
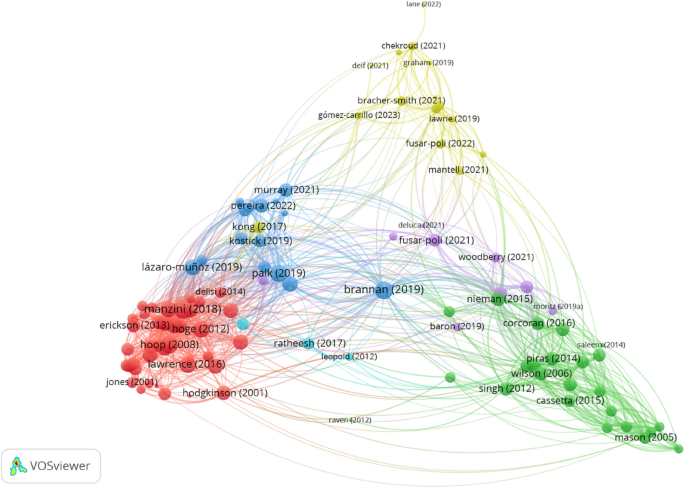
Map of bibliographical coupling relations between the documents. Fractional counting was used and the minimum number of citations of a document was set to 5. Nodes (dots) and edges (lines) reflect the strength of the links between the items. Colour indicates membership into different clusters
The largest cluster (Cluster 1), in red,—consists of 40 papers and (bottom left corner in Fig. 1). The green nodes in the bottom right corner are papers assigned to a considerably smaller Cluster 2 (24 papers). Further, there are two clusters of equal size, namely 15 papers each—Cluster 3 (blue nodes right above Cluster 1) and Cluster 4 (yellow nodes in the top centre part of Fig. 1). The purple dots in the centre of the map represent Cluster 5 that consists of 10 papers. Finally, there is a tiny Cluster 6 that consists of only 3 papers.
In some cases the decisions made by the VOSviewer algorithm are difficult to interpret. For example, Cluster 1 consists of closely related papers that address several ethical issues of genetic testing in psychiatry. However, the papers in Cluster 2 seem to address the same topic, but they are put into a different cluster. On average, the papers in both clusters are published around the same time—the mean year of publishing is 2010.7 for Cluster 1 and 2010.2 for Cluster 2. At least a partial reason behind putting the papers into two different clusters might be the higher proportion of empirical papers in Cluster 1—more than a half (18) of all (30) empirical studies are assigned to Cluster 1. By comparison only three empirical studies are assigned to Cluster 2. Further, it is also not easy to see how the topics addressed in Cluster 3 differ from Cluster 1 and Cluster 2. The nodes of Cluster 3 are wider spread than the nodes of Cluster 1 and Cluster 2 and in the map it is located closer to Cluster 1. However, on average papers in Cluster 3 are published more recently (2020) than the papers in Cluster 1 and Cluster 2. Moreover, if one takes a look into the list of authors of the papers in Cluster 3 then it becomes obvious that for a considerable proportion of articles are authored by an overlapping team of researchers (see e.g. (27,28,29,30,31,32)). Therefore, although the papers in this cluster are more oriented towards issues in research ethics, their being in the cluster at least partly might be explained by the citation practices of the authors. By comparison, Cluster 4 and Cluster 5 present less problems of interpretation. The papers in Cluster 4 address the issues of using machine learning (ML) algorithms in psychiatry and they talk about them using the framework of precision psychiatry. This is also the most cutting edge cluster on the map—the average publishing year of the papers is 2021. Finally, the papers in Cluster 5 address risks of genetic information and especially stigmatisation.
A significant part of the articles included in the review focus on genetic testing/screening for mental illness risk. The word “genetic” is the most used word according to Atlas.ti word frequencies analysis of the documents included in the review (see Fig. 2).
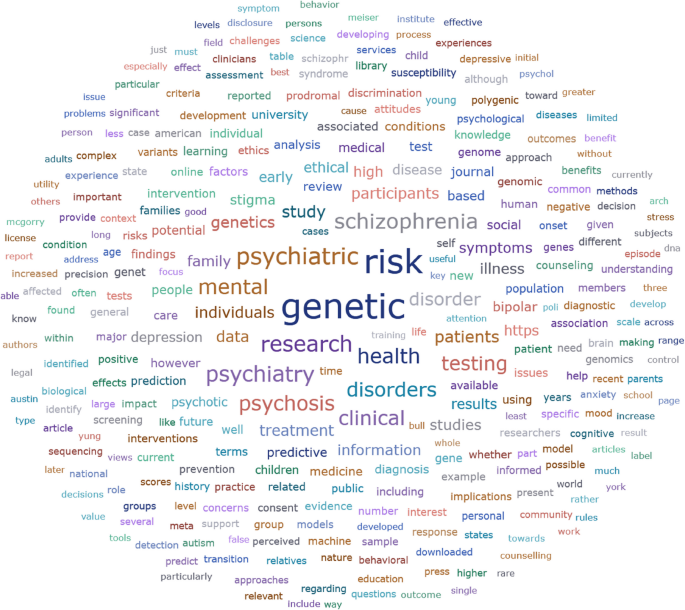
Results of word frequencies analysis
This might be explained by the attention that genetic testing attracted during the period the majority of the articles were written. Moreover, several papers use the term “genetic testing/screening” by not distinguishing specifically between diagnostic and predictive testing.
Qualitative thematic analysis of the included articles revealed four main themes: The themes and codes are presented in Table 3 and described in detail in the sections below (Table 3).
Potential benefits and harms
Benefits
Early prediction of severe mental disorders can bring several benefits. Some of them can be characterised as medical. For example, virtually all articles that discuss the benefits of predictive information point out that early risk prediction would enable the use of preventive measures and therefore reduce the risk or postpone the onset of a disease (33, 34, 21). This is highly relevant to children and adolescents (35). In case of psychosis risk prediction, the individuals may benefit from regular targeted follow-up which can help to detect the early signs of onset of psychosis. This also might help to minimise the duration of untreated psychosis which in turn improves clinical outcomes later (36, 37). Besides those effects, many authors emphasise benefits that are not (at least directly) medical. Some authors mention that predictive information positively affects the behaviour of persons. For example, the information on risks makes persons more willing to seek professional help and change their health-related behaviour (38, 33).
A rather long list of potential benefits from a series of qualitative and quantitative studies on genetic testing of familiar risk of a psychiatric disorder is compiled by Meiser et al. (39). All studies included in their review (except one which involves research participants who have undergone genetic testing for risk) are based on hypothetical future genetic testing scenarios. The review indicates that there is a belief that genetic testing in adults may help individuals to accept their condition and make them more willing to seek treatment, monitor their behaviour and change it accordingly or avoid triggers. They also note that one of the most widely documented benefits of genetic testing is the “potential to engage in preventive measures” (39). Another important finding in the review by Meiser et al. is a belief that genetic testing might validate the status of mental illness alongside physical illnesses and this in turn could help to decrease social stigma that is associated with mental disorders. The rest of the benefits in the review might be subsumed under the category of control, namely, genetic testing improves the basis for planning for the future, i.e., the information might help people to make financial decisions, decisions about marriage and procreation, etc.
A qualitative study by Lawrence et al. based on semi-structured interviews with young adults at high risk for psychosis about hypothetical genetic testing provides some evidence that a test that indicates an increased genetic risk can cause positive emotions such as happiness and an increase in self-esteem (40). Manzini and Vears also point out that some authors have proposed that predictive psychiatric genetic testing in minors allows a family to be better prepared to recognize and prevent the illness, detect early symptoms, reduce anxiety and have positive effects on family relationships. For example, it creates an opportunity for the family to discuss the condition openly. Moreover, there is evidence that some parents believe that predictive genetic testing allows them to prepare better for caring for their at-risk child (35). Finally, several empirical studies indicate that there is a demand for predictive psychiatric genetic testing. For example, Laegsgaard and Mors in their study of psychiatric patients and their relatives report that 83% of the patients and 75% of relatives would choose to have a genetic psychiatric test, some of them (38% and 30% respectively) even if there are no options for a treatment. (41) They point out that other studies have reported similar results—“All in all, 75–99% of respondents in these studies express positive attitudes toward psychiatric genetic testing, indicating a highly positive attitude to psychiatric genetics among persons suffering from bipolar disorder or schizophrenia (..) and patients suffering from a broad range of mental diseases”(41). Meiser et al. report a similar result. In the studies of adults they have reviewed, between 63 and 85% of participants expressed either willingness to test or a positive attitude towards testing (39).
Risk of misinterpretation and bias
When discussing the development of polygenic risk scores for prediction of mental illness, several authors emphasise the importance of using diverse and inclusive samples to avoid creating inequalities in the predictive accuracy of the models (13, 8, 42, 43, 29, 44, 23). As Palk et al. observe, “the majority of GWAS have been conducted in high income countries, and, even within these contexts, have included mostly participants of European ancestry”(42). As a result, the predictive accuracy of the polygenetic risk score is much higher in these populations. This problem is exacerbated further when machine learning algorithms used in the prediction models are trained only on the same populations. This issue is discussed below.
Further, another concern is the risk of false positives and negatives. False positives are prone to change the risk–benefit ratio of risk prediction by subjecting individuals to unnecessary risks without bringing any benefits. Corcoran et al. note that in the case of screening individuals at risk, false positives create a risk of over-treatment (45, 22). Individuals are unnecessarily exposed to the stigma of provisional diagnosis (21) and other harms, such as anxiety and “needless avoidance of developmentally appropriate challenges” (46). Lawrie et al. add to the list also potential negative consequences for employment and obtaining insurance, adverse impact on relationships, self-imposed restrictions, prejudice and discrimination (47). That said, there are also risks of false negatives such as delayed treatment, exacerbating the condition through illicit drug use and stress (47) and a false sense of confidence (48).
Some papers raise concerns about mistakes made in the interpretation of the results. So, for example, Chapman writes that regarding the use of polygenic risk scores, the potential of mis- or overinterpretation by healthcare providers, patients and consumers is a significant challenge (43). The consequences of that might be overdiagnosis and overtreatment. Several conditions can contribute to misinterpretation, e.g., individuals may lack necessary probability literacy and risk numeracy (43, 49), and they overestimate the role of genes in causing the condition. In other words, as a consequence of learning more about genetic predisposition people may disproportionately discount the role played by environmental and lifestyle factors (43). Ahlgrim et al. suggest that “high-risk populations are inherently vulnerable to having their judgment clouded by the promises of preclinical detection” (50). This might create unjustified optimism and unrealistic expectations about the benefits of testing and early interventions (49). It is worth to note that these consequences are mostly theoretical speculations of the authors. This does not mean that they are unfounded. But there is a good reason to justify them with empirical data.
Risks of AI use
The risks of AI use in the prediction of severe mental disorders are not addressed as extensively as other topics. The reason for this is obvious—the ethics of AI use in medicine is still in its infancy. Most papers are concerned with implications of using machine learning algorithms and the resulting bias. Fusar-Poli et al. observe that ethical concerns are raised by “high complexity” and “poor explainability” of so called “black box” multimodal clinical prediction models, which “do not allow for backtracking of the key patterns that produced a specific prediction” (13). Martinez-Martin et al. raise concerns that physicians who do not know the rationale behind the generated predictions will not be able to assess and justify their treatment decisions (51). This in turn may jeopardises patients’ ability to give informed consent. Further, an increasing reliance on machine learning algorithms may turn them into something that is more than just support tools and encourages “defensive medicine at the expense of patient autonomy” (8).
Another concern expressed by several authors is that the machine learning algorithms reinforce already existing racial, socioeconomic and other biases (51, 52, 36, 53).
In the literature, this is called “algorithmic bias” (44). Already existing health disparities contribute to algorithmic bias and as Walsh et al. observe, if not prevented, this may create a “harmful feedback loop” when “existing disparities may lead to unrepresentative training data. This bias may seep into predictive models, which further exacerbate disparities owing to biased predictions for certain minorities and vulnerable segments of patient populations” (44). Therefore, for example, Lane and Broome claim that researchers must ensure that sample populations at every stage of research should be diverse and inclusive (8). Dwyer and Koutsuleris in their scoping review on translational machine learning for child and adolescent psychiatry note that such algorithmic bias has been demonstrated with real-world consequences for ethnicity and gender. Such mistakes must be “investigated and then mitigated or transparently described before model deployment” (54). This, however, is difficult due to the increasing speed by which the data is made available to researchers. As Fusar-Polli et al. observe: “The speed by which technology is making Big Data available to biomedical researchers is outpacing the development of new analytical techniques to understand the implicit process that leads to their generation” (13). Therefore, they suggest that in the process of development, validation and implementation of precision psychiatry models “bias-aware interdisciplinary research and innovative practices” will be necessary to avoid different biases. However, Martinez-Martin et al. note, that “with proper calibration, the algorithm can be used to reduce bias in health care” (51).
Finally, Starke et al. claim that the use of algorithms could cause harm directly, namely, by producing erroneous predictions. As an example, they mention the IBM’s machine learning-based computer system Watson which produced unsafe recommendations for treatment. Such errors, they say, are especially worrying if the algorithms’recommendations are readily accepted by physicians (53). This worry might be especially relevant provided the feature of the “black box” algorithms mentioned above—namely, the predictions of those algorithms are not transparent and cannot be assessed by the medical staff. Consequently, for example, Fusar-Poli et al. suggest that to increase transparency and ethical acceptability of predictions, transparent “glass-box” alternatives that are explainable and interpretable should be preferred (13).
Inequalities in access to health care
One of the concerns discussed is the cost-effectiveness of research and the implementation of predictive models into health care. The main concerns are whether the research and use of predictive models will be effective and sustainable (55, 56) and how their implementation might affect the overall distribution of healthcare resources in the already underfunded mental care (57, 13). At the moment there is no “solid demonstration of precision psychiatry over standard approaches” (13), but there are good reasons to expect that the costs are high, and subsequently will take away the resources from other modalities. This is a serious issue especially if one considers that in many countries mental health research and treatments are underfunded (58). Further, some authors have expressed concerns about the accessibility of the service to marginalised populations (13, 36). Moreover, as Fusar-Polli et al. observe: “Growing digital divides can also amplify disparities in the accessibility of clinical prediction models in economically disadvantaged and marginalised populations”(13).
Risk of discrimination and stigmatisation
Ethical issues around stigmatisation are most often discussed in the papers in our review (see Fig. 2). One of the most prominent concerns is the worry that testing for severe mental illnesses increases stigmatisation of the people at risk. Ruhrmann et al. note that “The risk of early stigmatisation, negative labelling, and stereotypes has been voiced repeatedly by the opponents of preventive efforts, especially with regard to early detection” (59). The concerns about increased stigmatisation in the context of early prediction are pressing as individuals with psychiatric disorders are highly stigmatised (60), more so than those who suffer from somatic disorders (61, 60) Some empirical studies indicate that genetic explanation of mental disorders tends to increase stigma, in particular—it tends to increase social isolation and reduce empathy and understanding amongst healthcare professionals (60).
Further, individuals with psychiatric disorders often suffer from self-stigmatisation, i.e., they internalise the stigma which makes them perceive themselves as less valuable. Brannan et al. refer to empirical evidence that the stress associated with mental stigma, including self-stigma can increase the rate of transition to schizophrenia. Moreover, self-stigma can demoralise individuals and demotivate them to pursue employment and other life choices (60). To avoid stigma, individuals try to conceal their mental health status which in turn might significantly impede their access to mental health care (60, 62). Besides, one must take into account associative stigma as well, which affects the family members of the individuals at risk. Marriot and Broome in their paper refer to a study, according to which “the prevalence of associative stigma might be as high as 86%, with family members reporting feelings of depression, guilt and shame” (22). Finally, as some authors point out, there is a risk that healthy individuals will be unduly labelled as being at risk, and they will be stigmatised and, probably, offered unnecessary treatments. This, as Marriot and Broome point out “could contravene the principle of non-maleficence” (22).
However, the picture seems more nuanced than that. Some authors claim that genetic testing in fact might decrease stigmatisation by promoting the idea that mental disorders have a biological component and therefore are similar to somatic disorders. For example, in a study involving individuals suffering from depression, some participants expressed the view that a genetic explanation decreases stigma associated with the condition and changes the way other people perceive depression (63). There is evidence that many psychiatric genetic researchers hold a similar view. In a study conducted by Erickson and Cho, the majority of researchers in the field of psychiatric genetics that they interviewed, expressed a belief that “greater biological understanding of BP (bipolar disorder), MDD (major depressive disorder), and schizophrenia will reduce the stigma” (64). In addition, understanding that those disorders are biological conditions like other somatic diseases “would help to reframe mental illness as a condition outside the individual’s control, thus reducing guilt or sense of responsibility” (64). Meiser et al. in their review found that the overwhelming majority of the studies looking at participant’s perceptions of the impact of genetic explanation on mental illness-related stigma show that individuals believe that a genetic explanation would alleviate stigma (39). Bartolotti and Widdows on the basis of similar evidence claim that “Testing can promote knowledge about a psychiatric condition and decrease stigma among those who obtain such knowledge” but admit that regarding the wider social context the stigma would remain a danger (65). However, Brannan et al. mention a systematic review which shows that public understanding of the biological component of psychological disorders has substantially increased since 1990, but this has not helped to reduce the stereotype of individuals with schizophrenia as socially dangerous. Moreover, the social acceptance of such persons has even decreased (60). Therefore, it still might be the case that the promotion of a biological explanation of mental disorders runs the risk of exacerbating stigma.
It is important, however, to bear in mind that—as Brannan et al. point out (60)—the majority of studies on mental disorder-related stigmatisation examine attitudes towards individuals with a mental disorder. It is likely that attitudes towards subthreshold or asymptomatic individuals would be similar, however, currently, there is not enough evidence for that.
A further concern is that stigmatisation is associated with risks of discrimination. For example, stigma explains part of the higher levels of unemployment than the general population in people with schizophrenia (60). Also there is the potential threat of discrimination by insurance companies (66,67,68, 13, 60). A study conducted by Nwulia et al. indicates that individuals of African descent are more concerned about the risks that genetic information can be used in discriminatory ways (69). Finally, Marriott and Broome raise concerns about the risk of epistemic injustice (22). The term is coined by Fricker and it refers to “wrong done to someone specifically in their capacity as a knower” (70). Due to negative stereotypes and stigmatisation people with mental disorders might be unjustly treated as less credible both when they give knowledge or interpret their experiences. The issue of epistemic injustice in psychiatry has been discussed by Crichton et al. (71), however, Marriott and Broome raise this concern, regarding the individuals at risk (22).
Risk of commercialisation
Somewhat surprisingly, there is relatively little discussion on the risk of commercialisation of predictive tests for severe mental disorders in the literature. Eleven papers mention the topic. The main concern expressed by is the premature commercialization of predictive tests for psychiatric disorders, benefitting the product owner while the tests lack the necessary precision (64, 43, 72, 73). Chapman raises another pertinent issue: the potential involvement of commercial entities in development or production of novel prediction tools that might lead to conflicts of interest (43). This concern encompasses the necessity of implementing appropriate oversight mechanisms to avoid influence of commercial interests—bias in training of end users, downplaying limitations of prediction tools or alternative options, influence on clinical decision-making etc.
But commercialisation is not the only worry. The psychiatric genetic researchers interviewed by Erickson and Cho expressed their concerns regarding direct-to-consumer testing because the currently available genetic predictive tests for bipolar disorder, schizophrenia and major depressive disorder are “weak and nearly meaningless”. Thus, if offered directly to the customers, several harms might be caused. At best, it would be a waste of their money, at worst—it would be a cause of worry, feeling doomed and stigmatised, which is especially harmful for a psychiatric patient (64). Further, some researchers expressed worries that direct-to-customer testing has a negative effect on the whole field of psychiatric genetic research as society would become sceptical of the entire field (64). Another worry voiced by researchers is that such testing is dangerous because “people do not have a broader understanding of the significance of the results” (64). As a consequence, people misunderstand the results and make wrong decisions on the information available to them (64, 73). However, few researchers were more optimistic about direct-to-customer testing. They pointed out that it would prevent scientists from “taking overly paternalistic approach toward the general public” and that it would allow people to make their own decisions about what kind of information they prefer to have (64).
Response to predictive information
Numerous authors have voiced concerns regarding the potential harm that may arise as a consequence to individual’s reactions to the predictive information. For example, Bunnik et al. discussing differences between genetic testing for psychiatric and somatic diseases point out that knowledge of genetic risks for psychiatric diseases could potentially undermine a person’s sense of integrity and well-being before the appearance of symptoms. Further, they mention that a positive test result itself might serve as a trigger event for the disease tested for and “the manner in which the disease is understood by the patient (e.g. “it is in my genes, therefore it is an inevitable aspect of myself”) is likely to reflect on and modulate the development of the disease itself” (61). Similar concerns are mentioned by other authors as well. Cassetta and Godhari point out that screening for psychosis vulnerability might have potentially negative effects on personal identity: “For example, persons who are identified as being vulnerable for psychosis may begin to adopt a “patient” identity, which may lead to further exacerbation of their current psychotic symptoms. The new label may impact their future goals and aspirations, the level of support received from family members and friends toward achieving their goals and aspirations, and their levels of anxiety, which could affect the ability to meet those future goals” (74). Gomez-Carrillio et al. claim that receiving prognostic information can considerably affect individuals’self-perception. Thus “diagnostic constructs and explanations” become a reality that in a significant way influences and determines an individual’s experience (75).
Lebowitz and Ahn report results of experimental studies suggesting that if people are presented with results of genetic susceptibility to depression, they tend to report having experienced more depressive symptoms in the past. They point out that this finding is particularly alarming because the current psychiatric diagnostic system very much relies on retrospective self-report of past symptoms, therefore “delivering personalized genetic information to patients may complicate the process of making psychiatric diagnoses” (76). Therefore, prediction of risk might not only cause harm to the individuals but also impact the validity of psychiatric diagnosis as well.
Rights and responsibilities
Informed consent, personal autonomy and agency
Informed consent of patients and research participants is a constant a subject of debate in medical and research ethics. Informed consent ensures respect to autonomy, voluntariness and shared decision making if it provides necessary information, opportunities for dialog and necessary support. Nevertheless, the context of the prediction of severe mental disorders brings forward a specific set of issues. One problem is the amount and content of information that should be given to the person prior to making the risk prediction to ensure informed and voluntary consent. As Lane et al. have observed, a predicted psychiatric condition may not be well defined as “many studies include a range of different diagnoses with varied treatments and prognoses under the outcome of psychosis”and predictions are “inevitably uncertain” (36). Prediction of risk requires that the person is provided with “clear, simple, understandable and concrete” (77) information about the purpose of risk prediction, its nature, benefits, risks, limitations, actionability and potential consequences for the individual and family. The information should be tailored to the needs and situation of a particular person. Also, it is advisable to stratify the consent, for example, by “asking them whether they want information that is clinically actionable, has reproductive implications, may affect life planning, etc” (78). The same applies to the information about prognosis and possible benefits and disadvantages of learning one’s risk status. Lane et al. claim that there is not enough empirical research examining how individuals might react to personal risk predictions and therefore there is a lack of information on how to disclose the information in a manner that maximises autonomy (36, 74, 68, 51).
Another issue is the complexity of consent and assent in case of minors. For example, schizophrenia has a typical onset in adolescence or young adulthood (79) which means that a considerable proportion of predictive tests will be conducted when the individuals are minors, i.e., will not be at the age to have the legal capacity to consent and consent will be sought from their legal guardians (74, 80). This raises the question of “whether and how children would be involved in the decision to be tested and in the discussion of results”? (81). In a qualitative study by Erickson et al., most individuals with a personal and/or family history of mood disorders expressed a wish to test their children before adolescence, however, most of them also indicated that they would not share the results with the child until adulthood or until symptoms developed (81). Cassetta et al. mention a principle that is widely accepted in many countries, namely, that if minors are barred from giving consent by law or persons are unable to consent due to their cognitive capacity, one should try to get assent for risk prediction (74). Even in cases where individuals have reached the legal age of consent, several authors point out that testing for severe mental disorders raises questions about the capacity to consent (36, 74). As Lane et al. observe, individuals at high risk of psychosis may have “significant levels of comorbid psychiatric disorders, intellectual disabilities, and subthreshold psychotic symptoms” (36). That, as they note, has the potential to impair the capacity to give consent, but they also emphasise that that being the case one should not draw any generalised conclusion about the decision-making capacity of individuals with mental disorders (36) and that being at risk “does not automatically mean that an individual does not have the cognitive capacity to provide informed consent” (74) Instead, they recommend evaluating each persons’ capacity individually rather than making assumptions (74).
Rights to know and not to know
Right to know and not to know one’s genetic risk is a topic that has been widely debated in the context of testing for somatic conditions. Therefore, one of the main questions raised in the literature on genetic testing for psychiatric conditions has been, whether the psychiatric context makes any difference. Can the arguments that are used for either pro or contra rights to know and not to know one’s genetic risk regarding somatic conditions be applied in psychiatry? (65) One argument used by defenders of rights not to know one’s genetic risk regarding somatic conditions is related to actionability. Namely, if there are no treatments or preventive measures available for the condition, then the benefits of knowing might be outweighed by the harms of knowing (65). An important dissimilarity strengthens this argument in a case of psychiatric condition. As some authors have argued, it is reasonable to consider that unlike in screening for cancer, the knowledge of being at risk of developing a psychiatric condition itself might play a causal role in developing the condition (82, 65). Thus the case for the rights not to know is made stronger.
Privacy and confidentiality
If novel risk prediction models are being implemented in psychiatry they will likely rely on a great variety and quantity of data. Therefore, privacy, data safety and confidentiality are a concern (13, 83, 84, 36, 56). As Manchia et al. point out: “given that precision psychiatry is strongly related to the analysis of massive datasets (either phenotypic, neuroimaging, or biological), confidentiality and privacy concerns are becoming increasingly relevant” (56). To mitigate these concerts they suggest that “it is crucial to develop an appropriate ethical-legal framework, which would facilitate safe data sharing” (56). In a similar vein, Fusar-Polli et al. warn about ethical concerns regarding “privacy, cybersecurity, confidentiality and device dependability” (13). In particular, they stress that “leaking of private information can affect personal lives, including bullying, high insurance premiums, and loss of jobs due to medical and psychiatric history” (13). They also suggest that “These concerns should be addressed by the implementation of strict data governance and security policies that comply with local regulations”(13). Lane et al. note that empirical evidence suggests that, for example, individuals at high risk of psychosis “feel apprehensive about information security and privacy of genetic risk information”(36). They refer to the study by Lawrence et al. which indicates that information privacy is an important concern for individuals at risk (40). Similar concerns are expressed by participants in a study conducted by Mantell et al (33).
Another concern regarding confidentiality is related to the involvement of the family members. Cassetta and Goghari note that provided that heritability is high for several psychiatric disorders: “it is conceivable that first-degree relatives of persons who undergo screening for psychosis would have a personal interest in obtaining the results of the screening procedure” (74).
Counselling, education and communication
Need for guidelines and standards
Several authors recently point out that the lack of guidelines is an obstacle to the implementation of different aspects of prediction of risk in psychiatric clinical practice. For example, regarding novel prediction models using AI Graham et al. point out that “there are no established standards to guide the use of AI and other emerging technologies in healthcare settings” (23). Ward et al. mention, that despite different potential applications for genetic testing in psychiatry, psychiatrists still face a “critical structural challenge”, namely “the lack of a clear standard of care and professional guidelines for the use of genomic testing and management of findings” (32). The lack of standards creates some problems already in the research phase. As Chapman indicates in her study, in the research of polygenic scores (PGS) every research group uses different methods to develop PGS and their results therefore can diverge. She refers to a study by Docherty et al. (85) in which they conclude that the current regulatory environment enables “oversimplification and exaggeration of research results for marketing purposes” and provision of genetic tests “without demonstration of clinical validity” (43). Ward et al. point out that provided quick development of psychiatric genomics and increasing use of testing in psychiatric practice one should expect a period of uncertainty about what constitutes a responsible use of these developing technologies. They emphasise the role of professional organisations in minimising the uncertainty by developing practice guidelines: “Such guidelines would help to establish a standard of care and would go a long way in addressing clinician concerns regarding proper practice and legal liability related to the use of genomics findings” (32).
Actionability
Most of the benefits of the clinical use of prediction of risk are dependent on the availability of clinical interventions that can either prevent or postpone the onset of severe mental illness. However, currently, these abilities are very limited and there seems to be a consensus that under such circumstances prediction of risk for a psychiatric condition is not advisable as it might cause harm without providing any clinical benefits (86). Empirical data indicates that individuals and families who are interested in testing at least partly share this attitude. Namely, as Meiser et al. report in their review, adults’ interest in genetic testing for psychiatric conditions depends not only on the predictive value of the test but also on the availability of treatment and/or prevention options (39). However, there is evidence that some individuals would be interested in testing notwithstanding treatment possibilities (63). Parens et al. find that a surprising result (87), but this might point to the importance of non-clinical benefits that individuals expect from testing. Moreover, it seems that the preventive measures should not be understood too narrowly. This point is emphasised by Fusar Poli et al. According to them, one might object that “if no effective preventive intervention can be provided, then knowing in advance may not be helpful outside clinical monitoring (which can reduce the duration of untreated disorder). However, young people accessing preventive (e.g., CHR-P) services benefit from an integrated package of vocational, psychosocial and familial support interventions which would otherwise not be available to them” (88).
Education of professionals and laypeople
For the successful implementation of prediction models in clinical practice, some basic knowledge of the technologies involved is essential for all the stakeholders, and even in-depth knowledge might be needed for professionals using them in clinical practice. However, several studies indicate that there are no good reasons to be optimistic in this regard. The study by Erickson and Cho suggests that the general public lacks understanding and education “surrounding the field of genetics” (64). They point out that “The majority of researchers were in agreement that not only is there a lack of genetic knowledge among members of the general public, but there is also great difficulty in understanding probability and risk” (64). This is an important issue, because in that case “even if someone is given information about his/her genetic risk for a psychiatric disorder, it is likely the results will either be meaningless or misunderstood by the patient”(64). Most likely the same applies to other fields involved in the novel risk prediction models, like, epigenetics and neuroimaging, as well as to the use of AI. Fusar-Poli et al. also mention this as an ethical challenge that should be dealt with (13). However, it seems that similar concerns apply to health providers as well. The experts in psychiatric research interviewed by Erickson and Cho “emphasised that this lack of genetic risk education is a problem not only among the lay population. Almost every genetic researcher interviewed (n = 25) strongly believed that the majority of physicians and health care providers do not have the adequate knowledge or experience to help patients interpret genetic test results or to put these results in the correct context of probability or risk”(64). Bloss et al. also mention the physicians’ lack of training and knowledge of genomics as a hindrance to adopting genetic testing in clinical practice (89). Use of AI or use and interpretation of epigenetic or neuroimaging data may pose similar challenges. Fusar-Poli et al. point out that what matters in the communication of risks is not only knowledge but also the methods of disclosing:”the ability to communicate the results of a risk prediction analysis ethically relies heavily on the competence, level of knowledge and training, and skills of the health professionals. (..) This appears particularly crucial for sharing behavioural genetics findings (..), given that the risk of misinterpreting results might increase the potential for discrimination and stigma”(13). Lack of the knowledge and understanding may become a serious obstacle also for obtaining a voluntary and fully informed consent.
Counselling and empowerment
As discussed above, individuals’and healthcare professionals’ lack of genetic literacy and other types of knowledge underscore the importance of counselling on results of risk prediction. As Appelbaum and Benston claim: “Optimal genetic counselling incorporates both education and encouragement, assisting patients in embracing their autonomy and understanding what sort of control they might have in managing their symptoms”(49). To underscore the importance of counselling, they refer to an empirical study by Inglis et al. (90) which shows that specialised genetic psychiatric counselling increases individuals’ sense of empowerment and self-efficacy. Lawrence et al. have conducted an empirical interview-based study with young adults at clinical high risk of psychosis and claim that their findings “validate the important role of genetic counsellors, who are well positioned to help persons understand the risks and benefits of getting tested, understand their test results, and decide whom to tell”(40). Evidence for the benefits of psychiatric genetic counselling is also provided by the study of Costain et al. (91) and described by Mundy et al. (92) However, Mundy et al. point to an important problem, namely, that the majority of the empirical studies are aimed at the adult population. Provided that the novel prediction models for familial risk might be used in children and adolescents, this is a relevant gap that should be addressed by researchers. Further, as Appelbaum and Benston observe, the role of counsellors in psychiatry has been rather limited up till now. Part of the reason for this is the small number of them, at least in the U.S. Further, they point out that many of the existing counsellors know little about psychiatric disorders (49). Mundy et al. point out that the number of genetic counsellors falls below the recommendations by the WHO. They mention that one strategy to reduce the reliance on counsellors might be to train other healthcare professionals the necessary skills and there is some empirical evidence that might support such a move, however, more empirical research is needed to study that (92).
Ethical issues in different applications
Reproductive choices and prenatal use
Prediction of risk for severe mental disorders might affect the reproductive choices that people make. Hoge and Appelbaum note that “Preliminary studies suggest there is substantial interest in prenatal testing for other neuropsychiatric disorders such as bipolar disorder (..), schizophrenia, alcoholism, attention deficit disorder and depression” (78). They suggest that the high level of interest in testing “may reflect a lack of understanding of the likely value of predictive testing”(78). Laegsgaard and Mors surveyed the attitudes of patients with psychiatric diagnosis, their relatives and medical and psychology students and report that the support for prenatal testing is weaker than for testing of children or self (41). Moreover, the participants showed less support for prenatal testing for psychiatric than for somatic illness. They point out that similar results are reported in a study conducted by Smith et al. (93) in which they measured the intentions of bipolar patients, medical students and psychiatric students regarding termination of pregnancy in a case of a positive predictive genetic test result. The proportion of those participants who would terminate pregnancy for risk of severe life-threatening disease was higher than those who would terminate pregnancy for risk of bipolar disorder. Smith et al. think that this result can be explained by the fact that somatic diseases are perceived as potentially more fatal than bipolar disorder (93). A recent systematic review by Meiser et al. paints a similar picture. The studies included in their review report that attitudes towards prenatal testing were less positive than those to testing of adults or children. Further, “The observed trends indicate that the decision to terminate a pregnancy may be influenced by the likelihood of the condition as well as the anticipated severity of the disorder”(39). The reasons mentioned for the lack of support for prenatal testing were: “being against pregnancy termination in general, not considering the condition (e.g., bipolar disorder) as serious enough to warrant termination, not considering termination because of the increasing number of treatments that are becoming available, and the view that prenatal testing and selective termination could deprive humanity of the positive effects of bipolar disorder, such as increased productivity and creativity”(39). Some authors have expressed concerns that prenatal testing for psychiatric conditions would be conducted for eugenic purposes (64, 94, 42, 95).
Use in minors
Hoge and Appelbaum have raised the concern that “Parents may seek to have their asymptomatic children tested for susceptibility to disorders that might appear later in life, invoking their right to know their children’s vulnerabilities and to make family decisions”(78). They argue that this would go against children’s interests as they would not get any immediate benefit and in addition to that their “choice whether to be tested later in life will be pre-empted” (78). Meiser et al. in their review mention that the studies conducted to assess attitudes towards predictive psychiatric genetic testing for children show that interest in testing ranges from 61 to 83% (39). Not surprisingly, interest among patients was stronger than interest among at-risk relatives. The main concerns raised by testing children are the potential harms that testing can bring. The participants of the studies reviewed by Meiser et al. have expressed the concern that knowing about a child’s risk will cause anxiety. Some participants feared that the knowledge alters parents’behaviour towards their children and contributes to “child’s risk of developing psychopathology in the future”(39). Hoge and Appelbaum speculate that parents of a child identified as being at risk may allocate resources for education to their other children or try to protect the child thus affecting its development or self-image and that the test results may lead to discrimination (78). Morris and Heinssen point out that adolescents”may be impacted by greater responsiveness to peer pressure, altered risk perception, and increased focus on short-term risks and benefits” (80). As a consequence “these tendencies can affect adolescents’ thinking about their risk of developing illness as well as their risk of experiencing discomfort or adverse outcomes related to participation in a research study or clinical intervention”(80). Lane et al. mention the view shared by several authors that “In the field of clinical genetics, predictive testing of minors for adult-onset conditions is contra-indicated unless interventions in childhood can prevent or ameliorate illness”(36). They point out that the ethical reasoning used to justify this view relies on the respect of children’s future autonomy and the concept of the right to an open future. Lane et al. claim that “In the case of psychosis prediction it is uncertain whether the therapeutic gain from pre-emptive interventions in childhood or adolescence is compelling enough to justify restricting future autonomy in this manner” (36). Manzini and Vears argue against this view. They claim that the argument about future autonomy presumes that “individuals suddenly become self-determinant when they reach the age of majority (often 18 years)”(35). Minors, they argue, do not constitute a homogenous group. Children develop and that means that”some individuals below the age of majority have the intellectual capacity and the emotional maturity to make competent decisions themselves” (35). Besides this, they also argue that the benefits of testing in minors should not be conceptualised too narrowly and there is some evidence that indicates that testing may reduce anxiety and have positive effects on family relationships. Regarding the use of prediction of risk for psychiatric conditions, it could be relevant to take into account the point of view of minors themselves. Empirical studies conducted on this topic indicate that minors are interested in predictive testing. The study conducted by Pavarini et al. involving 80 UK adolescents aged 16–18 years, found that”most participants were interested in taking a mental health predictive test, especially for anxiety, learning difficulties and depression”(96). They point out that their results align with other studies”showing adolescents value learning about themselves and their health” (96). The participants were specifically motivated to take the tests if they saw that the information provided by the tests was relevant to them due to their family conditions or symptomatology. This, as Pavarini et al. claim, “is supported by prior research that documented high interest in learning about one’s risk among individuals at clinical high risk for psychosis and those with familial experience of depression”(96).
Family and relatives
An ethical issue that is discussed regarding prediction of risk in the context of family is whether there is a duty to share the results of testing with other members of the family. The question has previously been broadly discussed in the context of testing for somatic conditions and whether testing for psychiatric conditions can be treated in the same way. Appelbaum claims that concerning testing for somatic disorders the duty to warn a relative about the test result is conditional on three factors: “1) the likelihood that family members are at risk; 2) the severity of the potential consequences; and 3) whether effective interventions exist to mitigate the risk”(97). He argues that it will be much harder to justify a duty to warn in case of genetic testing for psychiatric disorders because “the presence of one or more alleles associated with a disorder is likely to lead to only a modest absolute risk, the disorder itself will be treatable to some considerable extent, and preventive measures are likely not to be available” (97). DeLisi also points out that the duty to inform is much less clear in the case of risk factors of schizophrenia as the risk of developing the condition for relatives is, although increased still rather low (48). Daws concurs, saying that “Clinically, the duty to inform is made less potent by schizophrenia’s unique association with cognitive ability, which should be factored into deciding whether or not to apprise a patient of their risk”(55). Appelbaum suggests that a “more reasonable and less intrusive” way of action would be to advise the patient on the possible risks to his or her family members (97). At the same time, there is evidence that a considerable proportion of individuals actually share their test results with their close ones. Meiser et al. refer to a study by Potokar et al. (98) according to which “the majority of people (78%) with serious mental illness would share their genetic testing result with family and friends” (39). Another study they mention (40) involved individuals at high risk of schizophrenia considering hypothetical genetic testing. According to the results, the participants “would tell people with whom they felt comfortable and whom they trusted about their genetic risk”(39).
Research ethics
As novel tools for predicting mental illness risk are still under development, the review highlights specific ethical and social issues in the research context. A research study begins with selecting the research topic, a step that inherently ethical considerations. Then it is followed by recruitment of research participants, and the researchers have to ensure that the potential research participants fully grasp the implications of participation—in this case implications of testing mental health risks.. In a 2004 paper on ethical issues in psychiatric genetics Appelbaum raises the question ‘what should research participants be told about the results of the tests they undergo?’ bearing in mind that, e.g.,”(m)ost of the purported associations of genetic loci with psychiatric disorders have subsequently been disproved” and in the context of genetics absolute risk from a single allele is expected to be minimal (97). Around the same time, Biesecker and Peay discuss the importance of genetic counselling for research participants who are receiving genetic test results on the risk of psychiatric illness (99). A decade later Bieseker returns to the topic and emphasises that “An important aspect of consenting to these studies is an appreciation for the degree of uncertainty”, including the risk of false positive and false negative research results (100).
Another question is how to deal with incidental and secondary findings that are expected to emerge in the context of research due to the extensive genetic and other types of data analysed (50).
